Bridget Churchill explains how Spex Seating can adapt for Stroke (CVA) survivors.
[Insert picture of Bridget]
An article written and compiled by Bridget Churchill.
A stroke, or cerebral vascular accident (CVA) is a significant cause of deaths and disability world-wide. A stroke is caused by reduced blood supply to the brain. Statistics relating to stroke in the UK are listed below (Public Health England, 2018; Stroke Association, 2018):
- Most strokes occur in older persons (around 59%), over a thirdof first-time strokes happen in middle-aged adults (40-69 years)and 3% of the total estimated strokes occur in persons under 40years of age. Children can also have a stroke and around 75% ofthese are in children under 10 years of age and these affect further physical and cognitive development.
- Men are more likely to have a stroke compared to women andwomen tend to experience worse psychological and physicalrepercussions from stroke.
- A high number of stroke survivors will need post-acute care, a quarterof all stroke survivors live alone after a stroke and 45% of all strokesurvivors feel abandoned when leaving acute care (hospital).
- Evidence suggests that not all stroke survivors have beenadequately assessed for all appropriate therapies and with agreedgoals when they are discharged from hospital. There is also a riskthat access to wheelchairs may be limited poststroke (Frank, 2018).
- Stroke recovery can take place over several years althoughthe biggest steps in recovery are generally seen in the fewweeks after stroke.
[Image]
There are Two Types of Stroke:
- Ischaemic strokes occur when the blood supply becomes blockedto the brain, which causes brain cells to die. The effects of this typeof stroke are variable depending on the location of the damage inthe brain.
- Haemorrhagic strokes are caused when a blood vessel burstswithin the brain (intracerebral haemorrhage) or on the surface ofthe brain (subarachnoid haemorrhage). Haemorrhagic strokes aregenerally more severe, and these are more common in children.
The Effects of Stroke:
- Weakness of the muscles, difficulties coordinatingand performing activities.
- Impaired balance and postural control.
- Pain in the muscles and joints.
- Sensory changes (including numbness, pins and needles).
- Communication difficulties (including difficulties with understanding and expression)
- Fatigue and headaches.
- Cognitive changes, including reduced understanding, processing of information and awareness of the world and one-self.
- Visual difficulties.
- Continence difficulties (loss of bladder or bowel control)
- Psychological and emotional changes
Stroke and Associated Wheelchair Need
A high number of stroke survivors will require a wheelchair. This may be early on for mobility to or from activities whilst they are undergoing active acute and sub-acute rehabilitation but may also be required longer-term to accommodate for postural difficulties and ongoing weakness. The survivors’ wheelchair need poststroke can vary drastically depending on the type of stroke and the area of the brain affected. The wheelchair may be a manual or powered version or both.
Because recovery in the early stages can be quite marked, some survivors may no longer require their wheelchair prescribed once acute and community rehabilitation has discontinued (Garber, Bunzel, & Monga, 2002). Other survivors, although independent initially, may become dependent on a wheelchair at a later stage. It is important that wheelchair seating and support is offered to meet their immediate need and adaptable to changes that may occur.
When considering seating provision for stroke individuals, the key elements need to:
- Optimise posture for independent propulsion of the wheelchair.
- Provide appropriate postural support whilst optimising safe independent and assisted transfers.
- Supporting the body to maintain a healthy alignment against gravity at the hips, pelvis, trunk, and head.
- Support limbs in the presence of abnormal tone.
- Provide adequate postural stability to allow for upper limb activity in functional activities.
- Provide appropriate pressure relief and comfort.
- Provide support to minimise fatigue.
- Facilitate engagement in functional activities.
- Allow for adjustment and adaptation as needs change.
- Be easy to use by client and family/carers and minimise the risk of falls.
- Be aesthetically pleasing and allow for self-expression.
- Optimise posture for communication, swallowing and social interaction.
- Be able to quickly respond to changes in the stroke survivor’s functional ability.
- Facilitate inclusion in the wider social milieu to reduce social isolation.
- Be appropriate for either manual or powered wheelchair chassis.
Why Spex?
Spex seating is a versatile, adjustable modular system that can be fixed onto almost any wheelchair chassis (manual and powered).
The seating system can be transferred between different wheelchairs if the user requires this. It can be easily removed from the wheelchair chassis and transported. Users only need order what they need and can add/remove components as their condition changes.
There are paediatric, kids and adult seating technology ranges that can grow and adapt to the user as he/she experiences changing needs. Spex is customisable to reflect personal colour choice, easy to adjust and includes the ability to support complex and changing postures at any stage in life.
Spex shapes better lives and provides the right amount of support depending on need!
Spex Seating Technology Products
Spex for kids and adults is a modular seating technology system allows for easy adjustment and contouring for those with minimal to complex postural presentations. Products are customisable and can allow for rapid response to sequelae of stroke, such as hip fractures, muscle tone changes and range of movement changes at the joints.
Items can be used in isolation or as a full seating system on their chosen wheelchair chassis base. Seating technology products can be set up during the assessment ready for immediate use by the
user and can usually be fitted directly to an existing wheelchair chassis if the user already has one.
The Spex seat pan and backrest shell can be removed if the wheelchair and seating system needs to be transported in a vehicle (e.g. if fitted to a folding manual wheelchair).
Adjustments do not require specialist wheelchair clinics but can be done by locally trained therapists to optimise comfort and postural responsiveness to the users’ needs.
[Image]
Spex Head Support
The Spex head support range provides support in several different positions to provide optimal head alignment to encourage interaction, manage fatigue and pain and promote continued engagement in activities. The head support also offers proprioceptive feedback on the user’s head position in space.
[Image]
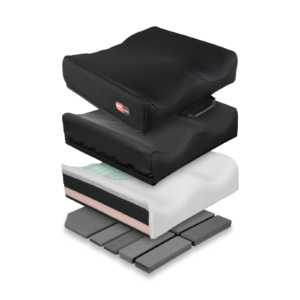
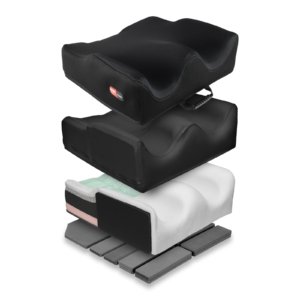
Spex Cushion Range
All cushions include both an incontinence cover and a fabric breathable layer. All cushions have an inherent Velcro fabric over the base to securely fix onto seat pans. Increased shaping allows for improved stability, reduced effort to sit to reduce fatigue, management of asymmetry and comfort for the user, and to support pressure management needs.
The Spex Vigour cushions provide a contoured cushion to promote comfort and posture.
The Spex contour cushions (contour, high contour and super high contour) have additional features allowing for shaping to the more complex postural presentation to promote stability at the pelvis, hips and thighs and promote comfort and pressure relief whilst influencing trunk alignment.
The Spex Flex cushion is designed to provide a stable base for those clients with a fixed hip asymmetry and obliquity. This cushion can promote a more upright posture in the trunk in sitting whilst accommodating hip flexion restrictions and can be shaped to accommodate/adjust obliquity.
[Image]
Spex Trunk, Hip and Medial Knee/Thigh Supports and Accessories
The Spex lateral trunk supports, hip and medial thigh/knee supports include patented axial technology that can respond to the user’s unique postural presentation and need. There are various sizes to suit individual need.
The configuration can be adjusted to promote safety with transfers as there are various mounting systems to suit independent, assisted and dependent transfer methods.
There is a range of pelvic support belts and thoracic support harnesses to optimise stability, posture and position within the seating system.
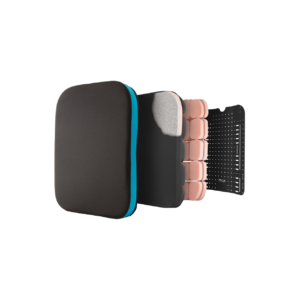
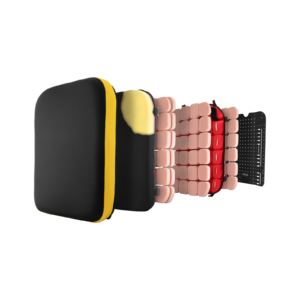
Spex Back Support
The height-adjustable shell option incorporates inbuilt growth adjustment in the back support due to the upper sliding interface.
The more supportive Spex and Spex SuperShape are versatile back supports that respond quickly (with easy adjustment) to more complex postural changes including posterior pelvic tilt or obliquity, spinal scoliosis. They are well suited to hypertonicity.
These back supports allow for greater immersion, pressure redistribution and support for those with marked asymmetry and complexity.
[Image]
The Spex Manta provides trunk support and allows for increase upper limb function when self-propelling or performing functional activities. It supports those with trunk weakness and can reduce side-ways leaning.
Shaping within these back supports is possible with the Spex Tesselated Positioning Kit and this kit can also potentially be used under other flat foam cushions to provide increased contouring.
[Image]
Contact us to:
- Arrange clinical education on our products in your venue of choice, or
- Obtain information about your local dealer for sales enquiries if outside of New Zealand & Australia.
[Insert PDF]
References
Frank, A. O. (2018, December 7). Rehabilitation of patients with stroke: summary of NICE guidance ignores powered wheelchair provision [Letter to the editor]. Retrieved from https://www.bmj.com/rapid-response/2011/11/02/rehabilitation-patients-st….
Garber, S. L., Bunzel, R., & Monga, T. N. (2002). Wheelchair utilization and satisfaction following cerebral vascular accident. Journal of Rehabilitation Research and Development, 39(4), 521–534.
Public Health England. (2018, February). Briefing document: First incidence of stroke – estimates for England 2007-2016. Public Health England Publications.
Stroke Association. (2018, February). State of the nation: Stroke statistics. Stroke Association. Retrieved from https://www.stroke.org.uk/resources/state-nation-stroke-statistics.