
Cerebral palsy (CP) is said to affect an estimated 17 million people worldwide and is the most common physical disability in childhood (CPAR Foundation, nd).
most common physical disability in childhood (CPAR Foundation, nd).
The severity of CP can vary from mild to severe and is a syndrome of motor impairment and is caused by damage to the developing brain. Damage can before, during and after birth due to infection or head trauma. “It is a group of permanent movement disorders that affect the development of movement and posture.” (Rosenbaum, Paneth, Leviton, Goldstein, & Bax, 2007)
Cerebral palsy related motor disorders can include muscle spasms, tremors, contractures, changes in muscle tone and difficulties with coordination and control of body movements. There are different types of CP (CP Alliance, n.d.) and these are diagnosed depending
on the area of the brain that is affected:
- Spastic unilateral CP or bilateral CP (characterised by increased muscle tone and stiffness in the muscles on one or both sides of the body).
- Dyskinetic CP (characterised by damage to the basal ganglia with difficulties controlling muscle movement; movements may be jerky, twisting or abrupt and unpredictable. These cannot be controlled and may become more evident when the person tries to move).
- Ataxic CP (characterised by difficulties coordinating movement).
- Unclassified CP or mixed CP.
The Gross Motor Function Classification System (GMFCS) helps to classify motor function for children (Palisano et al. 1997) between the ages of 0-2 years, 2-3 years, 4-5 years, and 6-12 years. For levels III – V the child is likely to require assistive devices for mobility. The environmental setting (home, school or the community) impacts on the level of independence with mobility and the need for mobility equipment (Palisano et al., 2003) and the greater the GMFCS the greater likelihood the individual require support for mobility at home, at school and in the community, although the preferred mobility method may be different between these settings (Palisano, Hanna, Rosenbaum, & Tieman, 2010).
As the GMFCS level increased, so too does the likelihood of asymmetric limited hip flexion, which further increases the prevalence of developing pelvic obliquity, trunk asymmetry, scoliosis, and windswept hip distortion (Ágústsson, A. et al, 2017).
Children with CP can present with instability of hip joints, with some children requiring surgery to manage this. Scoliosis may require surgery for realignment of the spine to optimise physiological functions such as digestion and breathing. Motor disorders of CP are often accompanied by other comorbidities such as problems with digestive tract motility, difficulties with eating and swallowing, increased risk of infection, reduced hearing and vision, and epilepsy. Pain and fatigue are common symptoms. Cognition can also be affected which can in turn affect behaviour and communication.
Cerebral palsy is a lifelong condition and emphasis for management should include the transition from childhood to adulthood, maintaining social inclusion and maximising quality of life (Colver, Fairhurst, & Pharoah, 2014). Rosenbaum et al. (2007) highlight that adults with CP emphasise communicating and being able to manage their environment as affecting their participation in life – this is something that requires focus throughout the person’s lifespan and the wheelchair needs to support this, if it is prescribed.
Wheelchair seating for children with CP has historically focused on maintaining anatomical and physiological wellness, but care must be taken to ensure that seating positioning also supports optimal engagement and performance within functional activities and is the responsibility of clinical team involved. The wheelchair needs to grow with the child, allow opportunities to engage and develop functional skills, optimise communication and comfort. When considering seating provision for individuals with cerebral palsy of school age (Costigan & Light, 2011), the key elements need to include:
- Optimise respiratory function.
- Reduce abnormal muscle tone and abnormal reflexes (such as asymmetric tonic neck reflex or labyrinthine reflex).
- Reduce risk and development of anatomical deformities of posture (kyphosis, pelvic obliquity, scoliosis, joint dislocation).
- Improve stability, safety and comfort.
- Improve participation and performance in functional activities.
- Ensure equipment promotes functional base of support and transfers to appropriate weight-bearing equipment
- Ensure lower body positioning and accessories support upper body alignment
Stabilising vision for school-based activities can be effortful for children with CP (Saavedra, Woollacott, & van Donkelaar, 2010) and seating solutions should consider the fatigue and effort required to engage in functional activities.
These elements need to be inherent at all stages and therefore seating solutions should:
- Support the body to maintain a healthy alignment against gravity at the hips, trunk, and head considering both body structure and function, activities and participation.
- Adjust to the pre- and post-surgical presentation and adapt to the person as their needs change.
- Include regular reviews to monitor for scoliosis and minimise secondary postural risks.
- Adequately support the pelvis and trunk to provide stability and allow movement of the head and limbs.
- Providing appropriate pressure relief, comfort and support to minimise fatigue.
- Facilitating engagement in functional activities and allow opportunities to develop motor skills.
- Be easy to use by client and family/carers.
- Be aesthetically pleasing and allow for self-expression as the child grows and develops their own identity.
- Optimise posture for cardiac, respiratory and gastrointestinal function.
- Be able to transition between manual and powered wheelchair frames depending on chair chassis required based on the person’s mobility requirements.
Spex seating is a versatile, adjustable modular seating system that can be fixed onto almost any wheelchair chassis and can adjust to the child’s changing needs. It can provide complex postural support, whilst still allowing for easy transportation, as appropriate. The same seating system can be transferred between manual and powered wheelchair bases.
The seating options include simple options to optimise comfort, as well as more immersive and shaped options to accommodate the need for additional stability and postural support. Spex is customisable to reflect personal colour choice, quick to adjust and modular to provide the right support when needed. Users only need order what they need and can add/remove components as their condition changes.
Spex shapes better lives and continues to adjust to the growing child’s needs.
The BINGO Spex provides the seating technology with the BINGO OT stroller- base. The child remains the focus when seated in the chair, whilst posture is well supported. Adjustments can be easily made as the child grows and as needs change.
seated in the chair, whilst posture is well supported. Adjustments can be easily made as the child grows and as needs change.
The BINGO Spex allows shaping within the back support and seat cushion to provide optimal support to a young child who may be demonstrating some of the musculoskeletal changes that occur with cerebral palsy, including hip instability and scoliosis. The accessories ensure that support is offered in the correct position for comfort and function.
Spex for kids and adults is a modular seating technology system which allows for easy adjustment and contouring for those with minimal to complex postural presentations. Products are customisable and can allow for rapid response to sequelae of stroke, such as hip fractures, muscle tone changes and range of movement changes at the joints.
those with minimal to complex postural presentations. Products are customisable and can allow for rapid response to sequelae of stroke, such as hip fractures, muscle tone changes and range of movement changes at the joints.
Items can be used in isolation or as a full seating system on their chosen wheelchair chassis base. Seating technology products can be set up during the assessment ready for immediate use by the user and can usually be fitted directly to an existing wheelchair chassis if the user already has one.
The Spex seat pan and back rest shell can be removed if the wheelchair and seating system needs to be transported in a vehicle (e.g. if fitted to a folding manual wheelchair).
Adjustments do not require specialist wheelchair clinics but can be done by locally trained therapists to optimise postural responsiveness to the users’ needs.
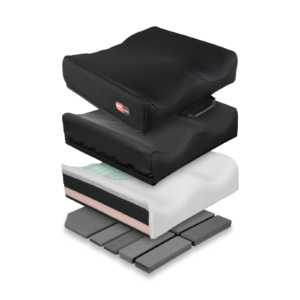
All cushions include both an incontinence cover and a fabric breathable layer. All cushions have an inherent Velcro fabric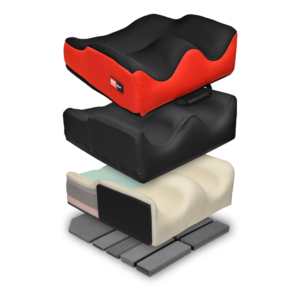 over the base to securely fix onto seat pans. Increased shaping allows for improved stability, reduced effort to sit to reduce fatigue, management of asymmetry and comfort for the user, and to support pressure management needs.
over the base to securely fix onto seat pans. Increased shaping allows for improved stability, reduced effort to sit to reduce fatigue, management of asymmetry and comfort for the user, and to support pressure management needs.
The Spex Vigour cushions provide a contoured cushion to promote comfort and posture.
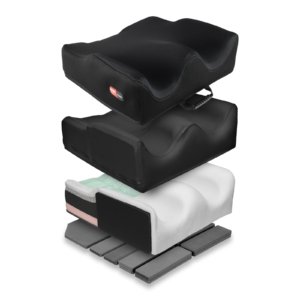
The Spex contour cushions (Standard contour, High contour and SuperHigh contour) have additional features allowing for shaping to the more complex postural presentation to promote stability at the pelvis, hips and thighs and promote comfort and pressure relief whilst influencing trunk alignment.
The Spex Flex cushion is designed to provide a stable base for those clients with a fixed hip asymmetry and obliquity. This cushion can promote a more upright posture in the trunk in sitting whilst accommodating hip flexion restrictions and can be shaped to accommodate/adjust obliquity.
The Spex lateral trunk supports, hip and medial thigh/knee supports include patented axial technology that can respond to the user’s unique postural presentation and need. There are various sizes to suit individual need.
The configuration can be adjusted to promote safety with transfers as there are various mounting systems to suit independent, assisted and dependent transfer methods and to reduce any falls risks associated with them. The axial technology can quickly adjust to pre- and post-surgical joint alignment of the hips and spine. Used in conjunction with the shaped back and seat supports, the modular seating system can be easily altered for immediate use.
There is a range of pelvic support belts and thoracic support harnesses to optimise stability, posture and position within the seating system.
The height-adjustable shell option incorporates inbuilt growth adjustment in the back support due to the upper sliding interface.
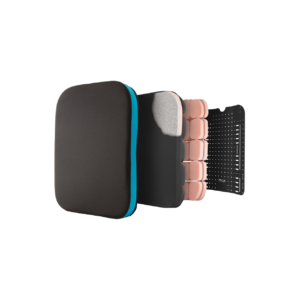
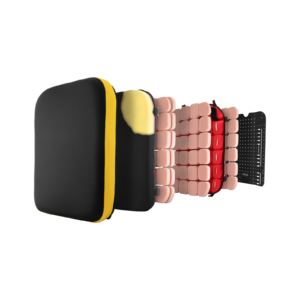
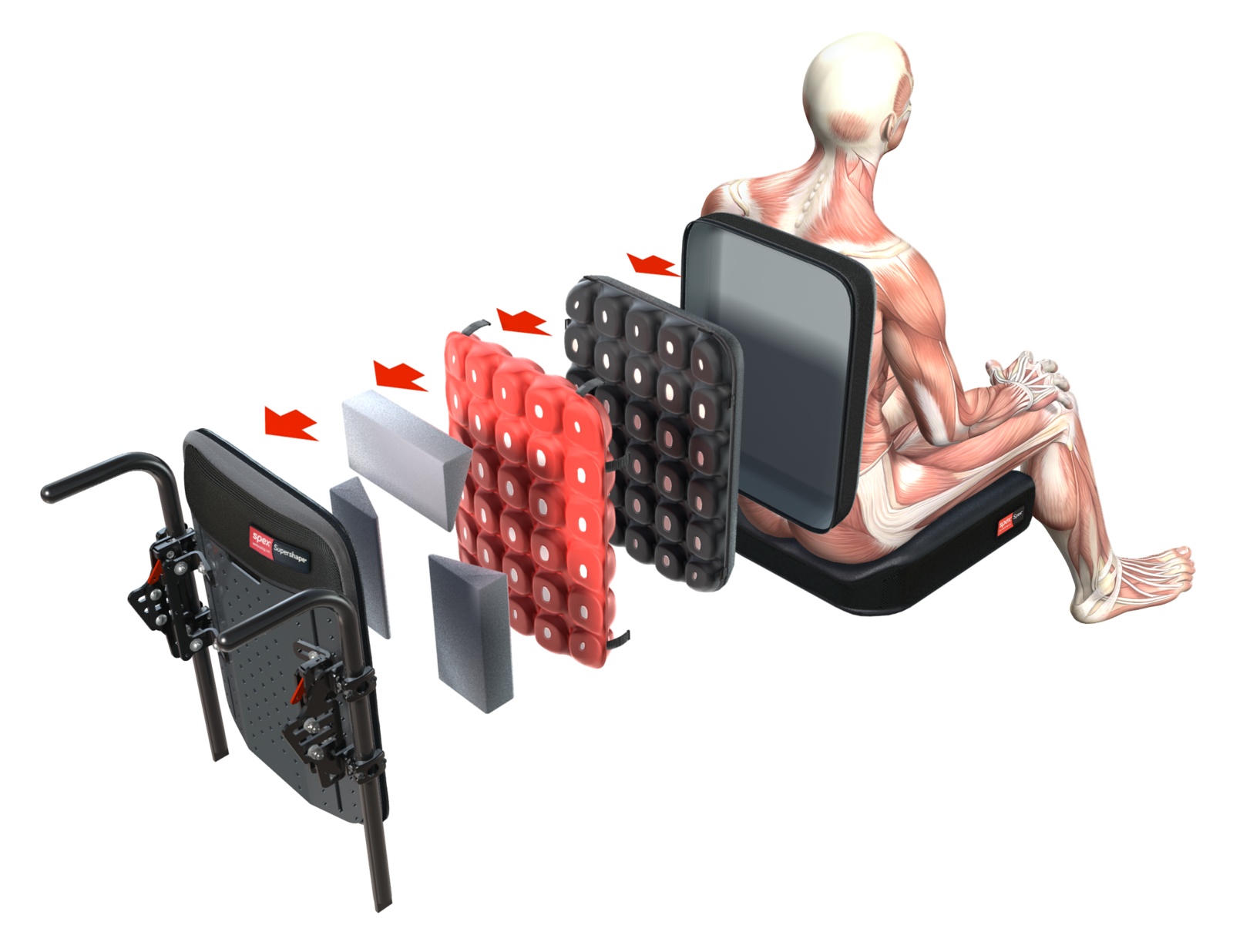
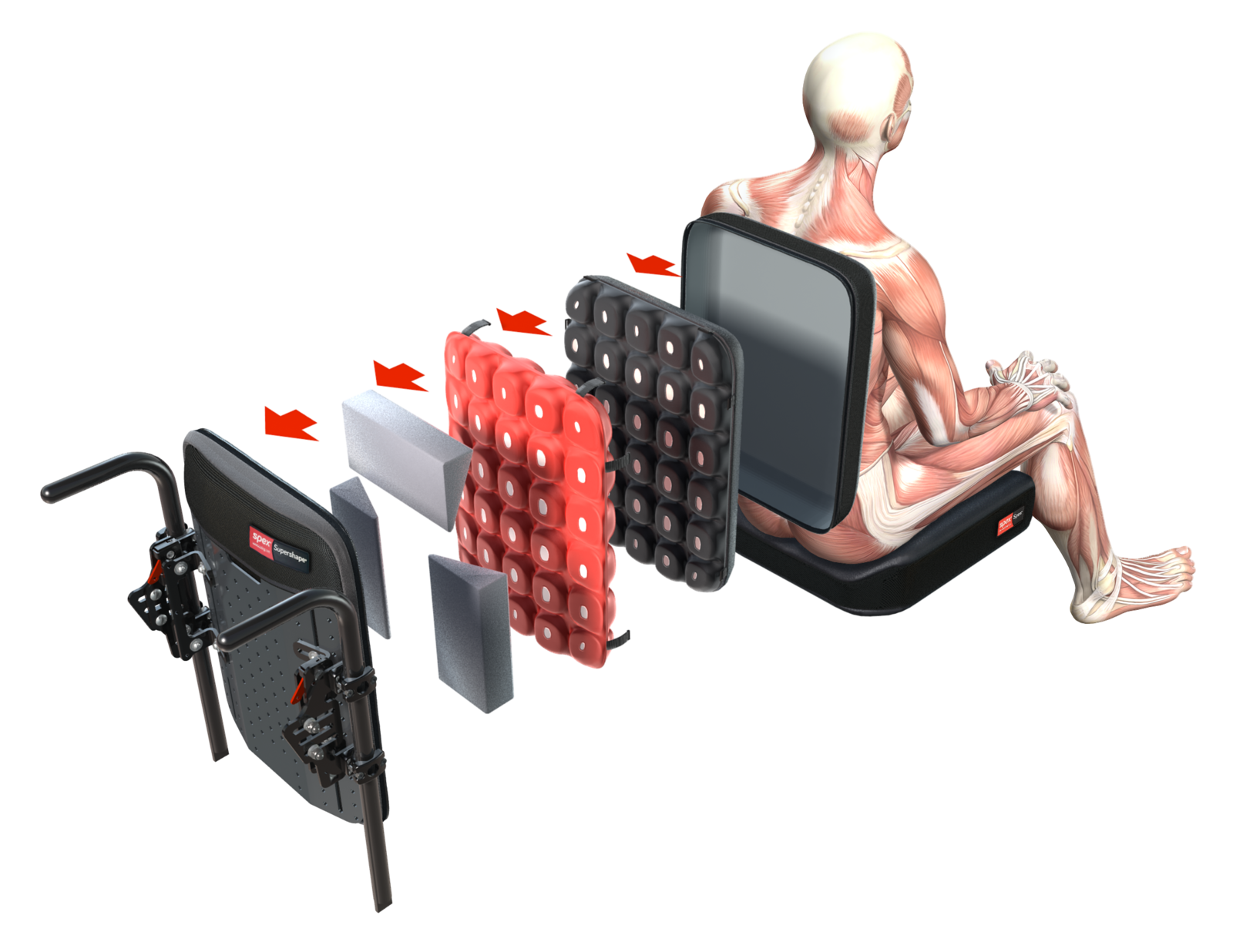
The more supportive Spex and Spex SuperShape are versatile back supports that respond quickly (with easy adjustment) to more complex postural changes including posterior pelvic tilt or obliquity, spinal scoliosis or asymmetry.
These back supports allow for greater immersion, pressure redistribution and support for those with marked asymmetry and complexity.
Shaping within these back supports is possible with the Spex tessellated positioning kit and this kit can also potentially be used under other flat foam cushions to provide increased contouring.
The Spex head support range provides support in several different positions to provide optimal head alignment to encourage interaction, manage fatigue and pain and promote continued engagement in activities.
The range includes the basic compact head support for users with good head control, the square head support, the contoured and the adjustable lateral head support for the more dependent user.
Contact us to:
- Arrange clinical education on our products in your venue of choice, or
- Obtain information about your local dealer for sales enquiries if outside of New Zealand & Australia.
Ágústsson A, Sveinsson Þ, Rodby-Bousquet E. (2017) The effect of asymmetrical limited hip flexion on seating posture, scoliosis and windswept hip distortion. Research in Developmental Disabilities, 71, 18–23.
Colver, A., Fairhurst, C., & Pharoah, P. O. D. (2014). Cerebral palsy. The Lancet, 383(9924), 1240–1249. https://doi.org/10.1016/S0140-6736(13)61835-8
Costigan, F. A., & Light, J. (2011). Functional Seating for School-Age Children With Cerebral Palsy: An Evidence-Based Tutorial. Language Speech and Hearing Services in Schools, 42(2), 223. https://doi.org/10.1044/0161-1461(2010/10-0001)
Foundation, C. P. A. R. (n.d.). What is cerebral palsy? | Cerebral Palsy Alliance Research Foundation. Retrieved 1 January 2019, from https://research.cerebralpalsy.org.au/what-is-cerebral-palsy/
Palisano, R. J., Hanna, S. E., Rosenbaum, P. L., & Tieman, B. (2010). Probability of walking, wheeled mobility, and assisted mobility in children and adolescents with cerebral palsy. Developmental Medicine & Child Neurology, 52(1), 66–71.
Palisano, R. J., Tieman, B., Walter, S. D., Bartlett, D. J., Rosenbaum, P. L., Hanna, S. E., & Russell, D. (2003). Effect of environmental setting on mobility methods of children with cerebral palsy. Developmental Medicine & Child Neurology, 45(2), 113–120.
Rosenbaum, P. L., Paneth, N., Leviton, A., Goldstein, M., & Bax, M. (2007). The definition and classification of cerebral palsy. Developmental Medicine & Child Neurology, 49(8), 1–44.
Saavedra, S., Woollacott, M., & van Donkelaar, P. (2010). Head stability during quiet sitting in children with cerebral palsy: effect of vision and trunk support. Experimental Brain Research, 201(1), 13–23. https://doi.org/10.1007/s00221-009-2001-4