This activity toolkit has been developed to educate therapists, carers and children with disability on the World Health Organisation and UK Chief Medical Officer physical activity guidelines for disabled children and adolescents, as well as the concept of 24 hour movement principles for optimal health.
The toolkit is intended be a resource for adapting guidelines to the unique movement abilities of children or teenagers with any type of disability, with some additional information for early years.
In the PDF format of this toolkit, all links in the resource sections are clickable hyperlinks intended to provide support to get more active, improve sleep, and link to worldwide guidelines and charity organisations for funding.
This toolkit has been greatly inspired by the brilliant work at the Canadian Disability Participation Project:

CHILDREN AND ADOLESCENTS
(aged 5–17 years)
In children and adolescents, physical activity confers benefits for the following health outcomes: improved physical fitness (cardiorespiratory and muscular fitness), cardiometabolic health (blood pressure, dyslipidaemia, glucose, and insulin resistance), bone health, cognitive outcomes (academic performance, executive function), mental health (reduced symptoms of depression); and reduced adiposity.
Good Practice Statements
- Doing some physical activity is better than doing none.
- If children and adolescents are not meeting the recommendations, doing some physical activity will benefit their health.
- Children and adolescents should start by doing small amounts of physical activity, and gradually increase the frequency, intensity and duration over time.
- It is important to provide all children and adolescents with safe and equitable opportunities, and encouragement, to participate in physical activities that are enjoyable, offer variety, and are appropriate for their age and ability.
In children and adolescents, higher amounts of sedentary behaviour are associated with the following poor health outcomes: increased adiposity; poorer cardiometabolic health, fitness, behavioural conduct/pro-social behaviour; and reduced sleep duration.
Physical Activity for Disabled Children and Disabled Young People




UK Chief Medical Officers’ Physical Activity Guidelines for Disabled Children and Disabled Young People 2022. This infographic was co-produced with disabled children, disabled young people, parents and carers.
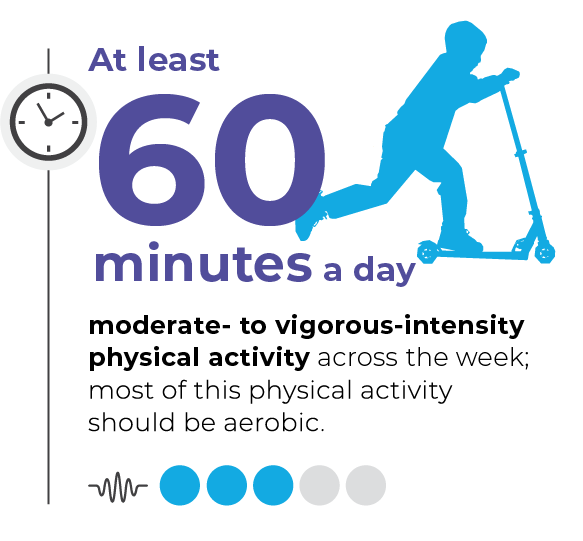
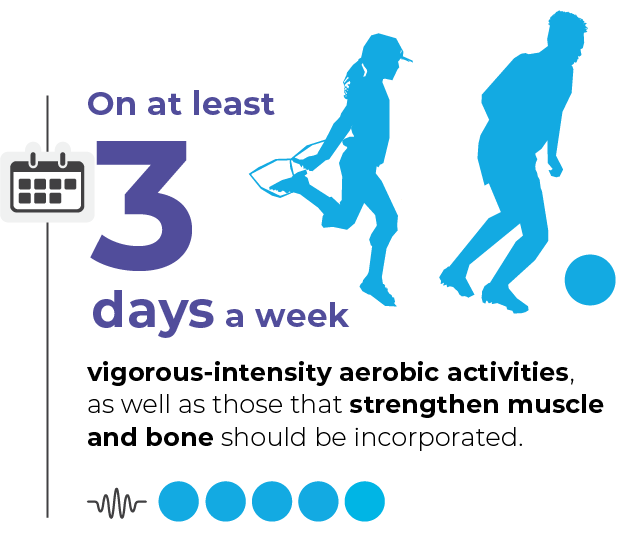
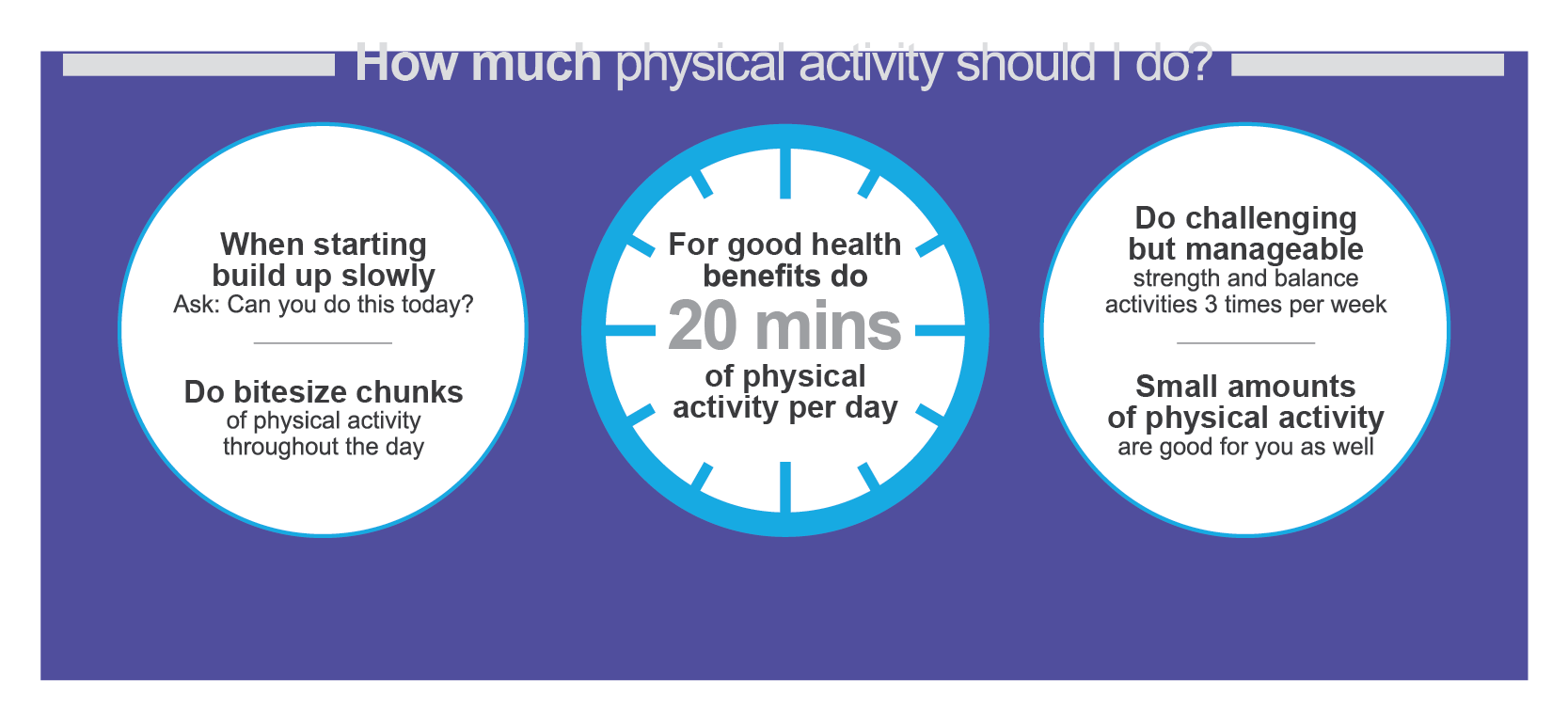
The UK CMO’s Guidelines advise children and young people with disability should undertake 120 to 180 minutes of aerobic physical activity per week, at moderate to vigorous intensity, which can be achieved in different ways – 20 minutes per day or 40 minutes 3 times per week. They also advise to complete challenging, but manageable, strength and balance activities 3 times per week. Activities could include, cycling, modified sports or yoga.
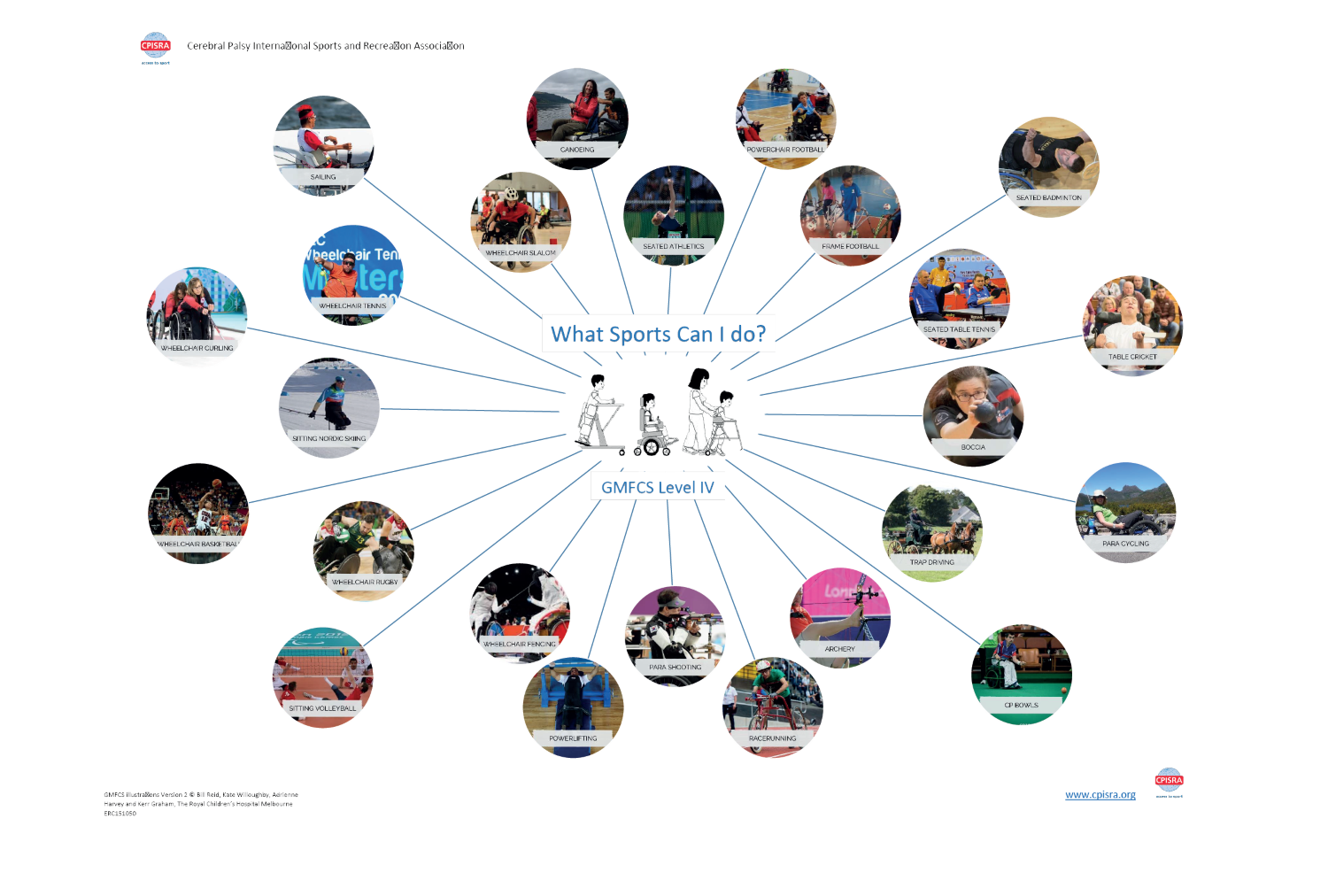
Moderate to vigorous physical activities require physical effort and should make you/your child or teen feel more tired and breathe harder than usual. Mobilising more often can be a great way to achieve more moderate to vigorous activity, and it’s important to remember that mobilising can be done in various ways – walking independently, walking with a walking frame, self-propelling with a wheelchair, using a tricycle. Try a variety of activities to find something you/your child enjoys. Being active together as a family can help make routines easier. A child or teen may not actually physically sweat when they do these activities. Useful resources can be found online, such as the ‘What Sports Can I Do?’ spider diagrams created by the Cerebral Palsy International Sports and Recreation Association:
https://cpresource.org/topic/exercise-sports-recreation/paralympic-sports-cerebral-palsy-athletes
International 24-hour movement guidelines for typically developing children encourage several hours of a variety of structured and unstructured light physical activities. Moderate to vigorous activity may be difficult to achieve and to measure, particularly in children with more complex disability. It may be more achievable to reduce high levels of sedentary behaviour with light physical activity. Remember, doing some physical activity is better than none!
Starting with small amounts of physical activity, and gradually building over time or doing bitesize chunks through the day can make it more manageable. Light physical activity requires smaller effort and movement of any body parts can equal light physical activity. Examples of light physical activity could be: playing games, painting, playing music, transferring in/out of an adaptive chair, household chores or getting washed and dressed. A change of posture and position, for example moving from sitting to standing in a standing frame, can equate to light physical activity!

International guidelines on sedentary behaviour for children and adolescents with disability emphasize the importance of limiting the amount time being sedentary. It is also advised to limit recreational screen time, such as watching T.V. or playing video games, but not including use of a communication aid or using screens for school work. Sedentary behaviour is associated with poorer health outcomes, so replacing this behaviour with light or moderate to vigorous physical activity is important. Remember, sedentary positions don’t have to be sedentary! Build blocks in an adaptive chair, play drums in a standing frame, paint whilst on a prone wedge! A child with disability should be supported to take many short movement breaks and postural changes throughout they day at school and at home.

Light physical activity
Several hours of a variety of structured and unstructured light physical activities.
Examples of light physical activities to try:
- Slow walking
- Boccia ball
- Household chores
- Finger painting
- Yoga
- Easy wheeling
- Building with blocks
- Drumming pots & pans
International 24-hour movement guidelines for typically developing children advise we should aim for between 8 to 11 hours of sleep dependent on age. Physical activity and sleep are likely bidirectional, whereby regular physical activity might improve sleep, and a more restful sleep with longer durations might positively affect energy/mood/cognition and enable more physical activity. Establishing routines such as regular bedtimes and avoiding recreational screen time or large meals before bedtime may be some simple starting steps to encouraging a more restful night-time period.
Use of sleep diaries can be helpful to monitor sleep routines and identify potential causes of sleep deprivation.
For those with 24-hour postural needs, a supportive sleep system may help improve sleep duration long term by supporting children in a symmetrical posture whilst asleep, reducing pain, improving pressure care and comfort.

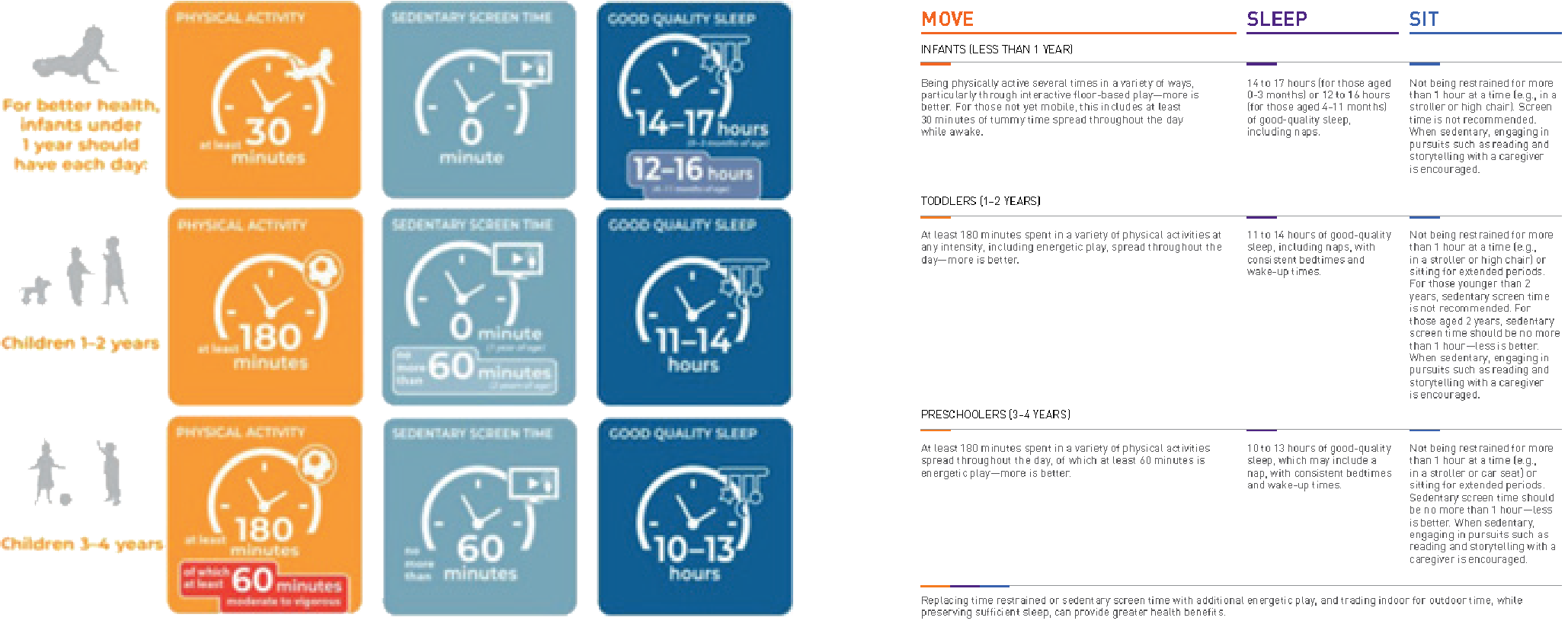
EARLY YEARS – The movement needs of children under the age of 5 are different to those of older children and
SLEEP adolescents, owing to the nature of a child’s growth and early development. Infants and toddlers require more sleep,
and physical activity should be based around play, development of skills, experience, and learning. Early childhood is typically a period of rapid physical and cognitive development and children and infants have remarkable brain plasticity and a natural ability to learn. A child’s habits are formed quickly and family lifestyle habits are open to changes and adaptations in infanthood. Forming good movement behaviours early on can help set up a good structure for later in life, as it is harder to change behaviour and routines that have already become established. Thinking specifically about postural care and physical developmental milestones, it should be encouraged that a child with physical disability is supported in experiencing the same movement as their typically developing peers, so long as it is appropriate, and any risks are managed. Expert clinical recommendations often encourage postural care programmes that encourage postural activity from an early age. Postural care in lying is recommended as soon as is appropriate after birth for the most severe movement impairments in those with Cerebral Palsy:
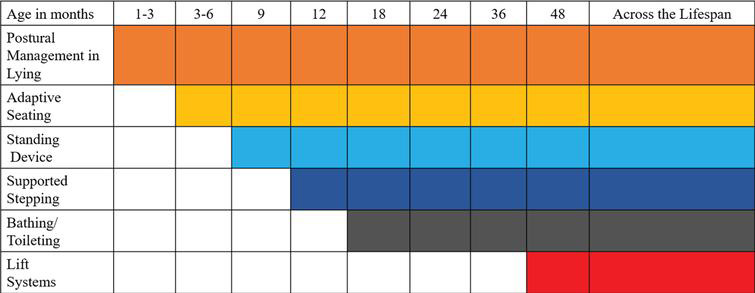
Image from: Paleg, G. & Livingstone, R. Evidence-informed clinical perspectives on postural management for hip health in children and adults with
non-ambulant cerebral palsy. Journal of Pediatric Rehabilitation Medicine: An Interdisciplinary Approach Throughout the Lifespan. 2022; 15(1): 39–48.
Support from a multidisciplinary team is therefore essential in ensuring an individualised programme is established for the child and so that families and carers can understand and engage in the benefits of early intervention, postural care and therapeutic equipment. World Health Organisation and Canadian 24-hour movement advice for children under 5:
 Ei Smart provide brilliant resources for age – appropriate play to support child development – and the leaflets are available in multiple languages!
Ei Smart provide brilliant resources for age – appropriate play to support child development – and the leaflets are available in multiple languages!
https://eismart.co.uk/resources/#podcasts-leaflets
Think about your typical daily routine/ the typical daily routine of the child you care for. How much physical activity, sedentary behaviour and sleep are you/they getting throughout this typical day?
Knowing what is vigorous or light physical activity can be challenging in children with disability, particularly those with more complex needs. It can also be difficult to remember exactly what activity you/they have done throughout the day. Therefore, it is encouraged that this 24-hour clock is completed in collaboration between the child, their carers, their health professionals, and their teaching staff.
Colour this 24 hour clock using the shading key provided to highlight the different levels of activity you/your child partakes in through the day. Remember as a general guide – moderate to vigorous physical activities require physical effort and should make you/your child or teen feel more tired and breathe harder than usual, light physical activity requires smaller effort and movement of any body parts can equal light physical activity, sedentary behaviour is a static activity with minimal body movement and energy use.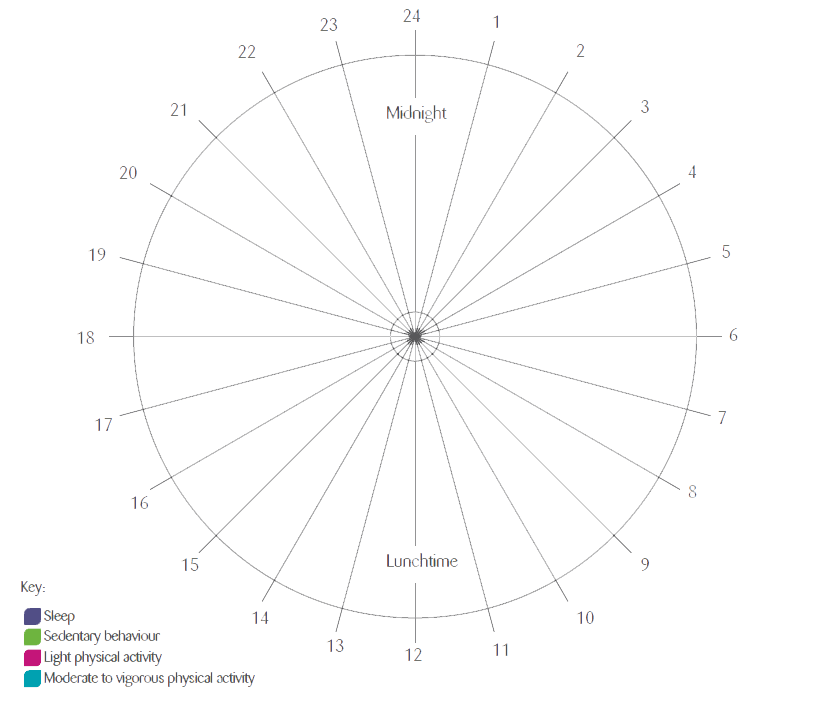
The F-Words build upon the World Health Organisation’s ICF Framework and includes key areas of a child’s development. Recognising that no one factor is more important than another, this can help guide clinical decision making and encourage more holistic, child and carer–centred approaches.